Treatment Planning
Frontiers in Breast Treatment Planning
Emerging techniques in breast planning offer alternative solutions for personalized treatment.
What the latest task group report includes regarding IMRT and VMAT secondary calculations—and what was left out.
As I suspected, that’s pretty much everyone. It makes good sense why: IMRT and VMAT employ MLCs and sophisticated treatment planning system algorithms to more precisely shape dose than previously possible. And this is precisely why these modalities are as ubiquitous as they are.
While they may be a clinical staple at this point, a task group regarding secondary checks for IMRT/VMAT only recently published a report providing some guidance addressing secondary calculations for these treatment modalities. A decade in the making, TG-219 establishes an approach for IMRT and VMAT secondary dose calculations.
In the span of those ten years required to publish the report, the community has settled into practice patterns of its own. Many of the recommendations may already be common practice as departments have independently developed best practices over time. So what does the new task group bring to the table?
These calculations are not intended as a catch-all but instead are designed to add to the integrity of the overall plan verification process. The task group strongly recommends that MU verification should not be used as a replacement for proper patient-specific QA. But having multiple methods in place provides a safety net that apprehends errors when they occur.
But secondary calculations have their limitations. For example, the dose reported to a single point isn’t necessarily representative of the plan as a whole. These calculations don’t catch machine delivery errors. And often, the algorithms used in these checks are more rudimentary than those used in primary calculations.
For that reason, parameters and inputs are often simplified to ensure the process is efficient. This may be changing as commercial options become available, and users adopt more robust and full-scale options. The task group distinguishes between types of algorithms, broadly categorizing solutions into factor-based or model-based approaches:
What TG-219 Forgot to Include
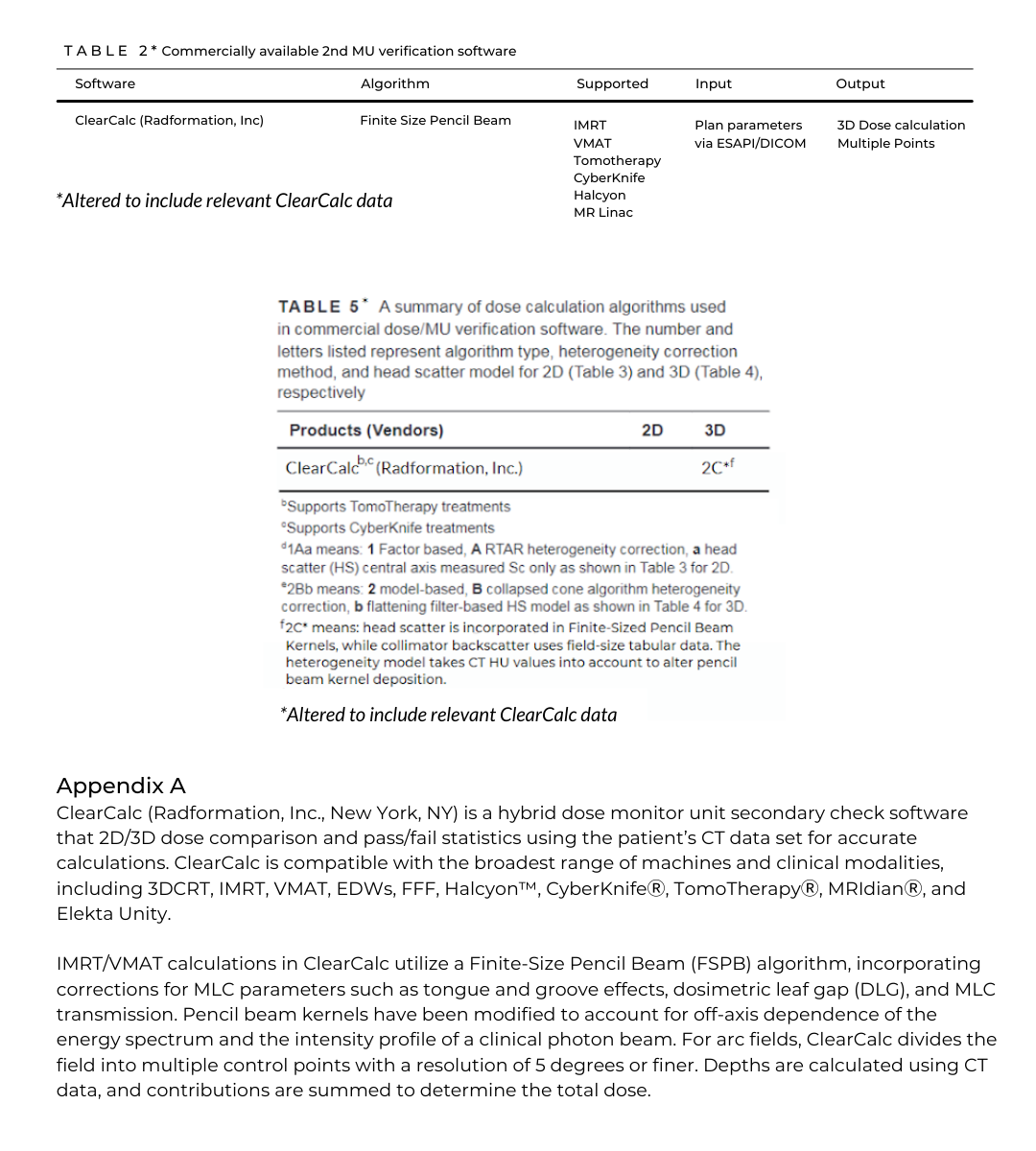
Unfortunate as that may be for ClearCalc users, that shouldn’t come as much of a surprise. After multiple years of work, the finalized task group report was submitted for publication in early 2021. ClearCalc wasn’t released until mid-2020, at which point final report iterations were likely circulating for approval.
Despite its relative youth compared to others in its class, ClearCalc quickly scaled to hundreds of installations in a short time frame. Given the adoption of Radformation’s secondary calculation software, we felt it was important to include additions to the published tables and appendix with ClearCalc-relevant data. This information is intended as a resource for clinics that use ClearCalc that would like to incorporate TG-219 recommendations.

Leave a comment