RadOnc News
The Focal Spot: Bette Blankenship
In this edition of the Focal Spot, Tyler Blackwell interviews Bette Blankenship, MS, FAAPM.
Does the future of medical physics involve more direct patient interaction?
The 2019 update to ASTRO’s seminal publication Safety is No Accident: A Framework for Quality Radiation Oncology Care suggests physicists play a role in patient and/or family education, a change from their recommendations originally published in 2012.

Some clinical physicists are already engaged, at least partially, in direct patient care. Wang and White assert in a 2019 Journal of Applied Clinical Medical Physics (JACMP) article that “while the logistics and practicality of assigning each patient a single medical physicist for the duration of their treatment seem both daunting and of dubious value, having the medical physicist interact directly with patients on a daily basis is common in our practice experience, particularly in brachytherapy, stereotactic procedures, isotope therapy, and the very common occurrence of solving set‐up problems in the treatment room.”
On the other hand, if physicists are filling time originally allotted for physicians to address similar physics-related questions and concerns, oncologists could reclaim this time for other care-related activities. This reallocation of time could actually lower patient costs.
But what about training? Soft skills? The educational background of a medical physicist includes limited patient contact—at best—as part of a residency’s clinical rotation. It could also be argued that physicists aren’t the best of communicators or even that we might potentially confuse patients further instead of clarifying difficult concepts.
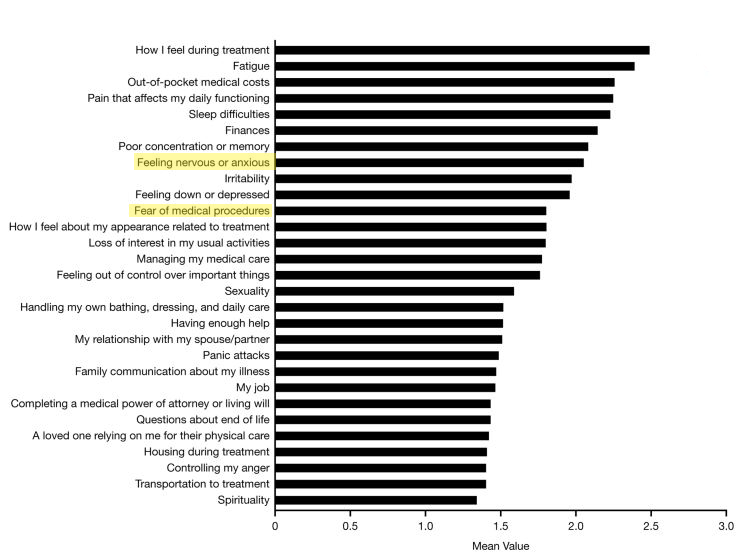
Some in the field are more optimistic about physicist inclusion in patient education prior to treatment. A study by Habboush et al. suggests there are legitimate gaps in patient education—ones physicists could potentially address. The study shows anxiety associated with radiation therapy “medical procedures” is higher than average when compared to other radiation treatment-related stressors. “Feeling nervous or anxious” is also a major stressor that ranks higher than average.
Physicist involvement in patient care clearly has potential to improve the quality of care for patients undergoing radiation therapy. But beyond that, the idea of increased patient-physicist interaction satisfies a number of the core strategic goals of the Medical Physics 3.0 initiative. Independent physics consults could benefit the profession as a whole by enhancing physicists’ visibility in the clinic and beyond. By interacting directly with patients, physicists can have more control of the technical process, earlier in the treatment timeline. Ultimately, carving out a new clinical role has the potential to expand the scope of practice for medical physicists, supporting the long term sustainability of the field.
According to Atwood, the idea of physics involvement in patient care came about as a result of an interaction he had as a resident at Stanford. “I was talking to a patient that was concerned and had a lot of questions. Her questions were by no means challenging, but you could just see how much more relieved she was after she got confident answers from a physicist. It completely changed the way she perceived her treatment,” says Atwood.
The UCSD Direct Patient Care Initiative team conducted a phase II trial published in 2018 that showed promising results. In addition to significantly decreasing patient anxiety, surveyed patients showed an increase in technical satisfaction leading up to the first treatment fraction. Overall patient anxiety scores were considered to be low at all questionnaire time points throughout their treatment. The response encouraged the group to continue their investigation with a randomized phase III trial which is nearing completion.
Admitting uncertainty about where this patient interaction might fit into a clinical routine, Atwood admits he and his team don’t have all the answers. “First we’ll try to show that this is beneficial, that it makes a difference, and then we’ll see how to best integrate it clinically. Realistically, it’s a while before this is something that is a huge component of everyone’s life and maybe not everyone needs to do it, but that doesn’t mean it might not be the right thing for our field,” he says.
What do you think? Will medical physicists play a greater role in direct patient care in years to come? Or is physicist participation in patient education an overblown and unnecessary abstraction?

Leave a comment