RadOnc News
TG-219: Secondary MU Calculations For IMRT and VMAT
What the latest task group report includes regarding IMRT and VMAT secondary calculations—and what was left out.
Emerging techniques in breast planning offer alternative solutions for personalized treatment.
But when new methods emerge, it’s worth considering whether these methods could improve (or replace) the status quo efforts. Below, we’ll introduce you to a novel technique for challenging boosts, discuss the merits of a method that has yet to reach its prime, and reveal which breast planning method wins the trophy for overall planning efficiency and effectiveness.
There’s a solution for that. A technique developed by Pearson, Wan, and Bogue at the University of Toledo makes one straightforward addition to their mini-tangents that dramatically improves conformality: a single arc.
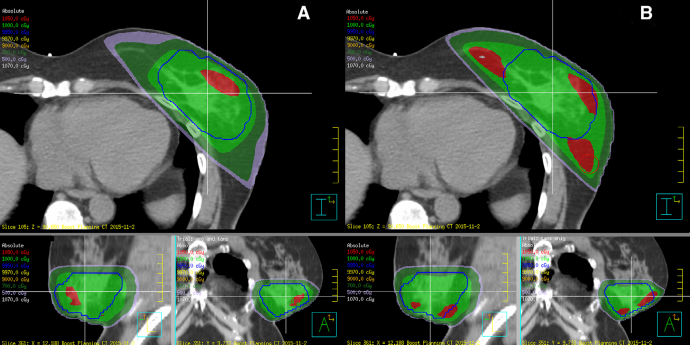
Of course, the sheer nature of the arc implies the delivery of a small amount of exit dose to surrounding structures. The ipsilateral lung sees slightly higher doses from this technique, as does the heart (more exaggerated for left breast cases). This tradeoff must be considered on a case-by-case basis, but ultimately, this new method for deep-seated seromas has potential.
Interested in planning with arcs using EZFluence?
We’re here to help. Email info@radformation.com and our support team will walk you through how to plan this technique using EZFluence.
Hybrid IMRT solves the large separation issue by pairing open fields and modulated fields to accommodate variation in body habitus. In this technique, high energies are typically used on the open field, allowing skin-sparing, depth penetration, and a reduction of hot spots, while the lower-energy modulated field creates homogeneous coverage of the target volume. While not a new concept (hybrid IMRT was described in a 2005 paper by Charles Mayo, et al.), implementation of the technique has lagged. But for those who are already using electronic compensation for breast planning, adding the open field component has its benefits.
The results showed marginal (but significant!) deviations for parameters such as conformity index and homogeneity index, while other metrics varied widely. The average time required for 3DCRT and EComp (14 and 15 minutes, respectively) was dramatically lower than that required for IMRT (36 min for tangents, 80 min for multi-field IMRT).
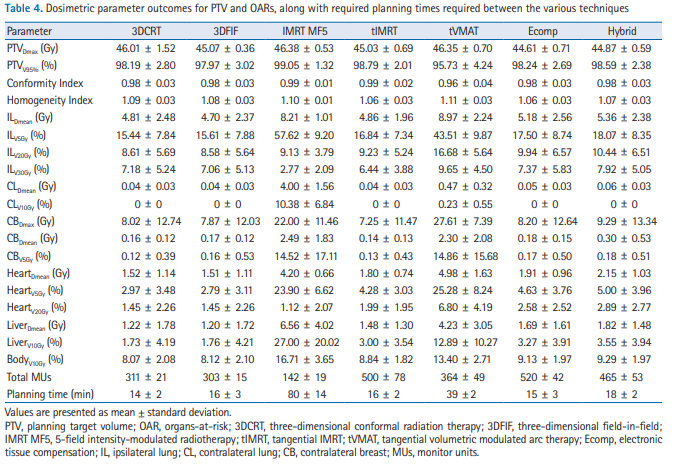
Some physicists reading this might take issue with this conclusion since this analysis only takes into account the time involved for these techniques in the planning phase. Many sites require patient-specific QA for EComp delivery, which may ratchet the sum total time investment required.

Leave a comment